
For this topic, I would like to introduce a practice that has been widespread internationally for over 20 years but remains relatively unpopular in Thailand—migraine and chronic headache surgery.
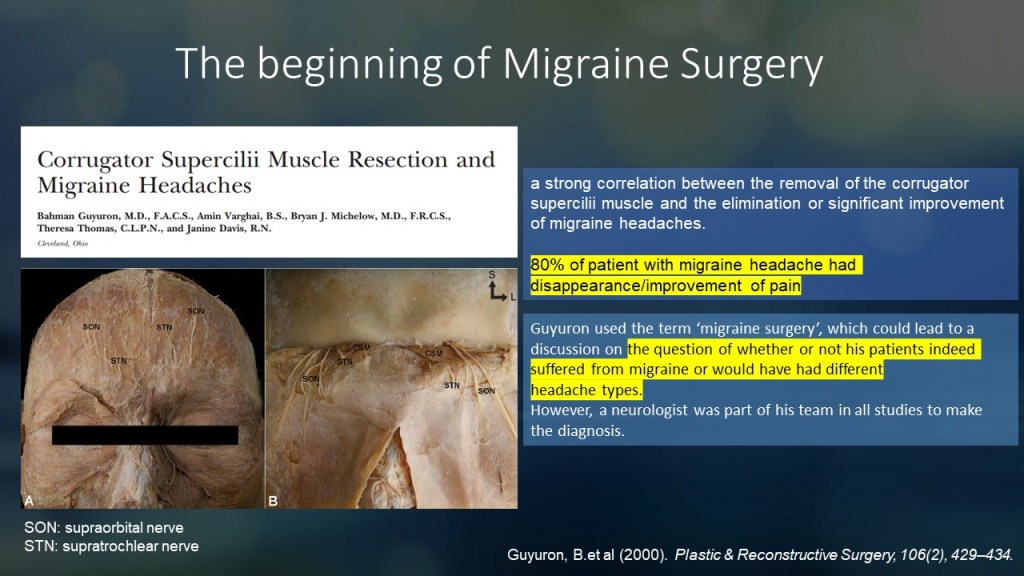
Migraine surgery originated from studies in patients undergoing cosmetic surgery in 2000. These studies, led by Guyuron and colleagues, examined patients who had surgery on the muscle around the orbital area called the corrugator supercilii.
This muscle is located around the orbital rim and functions to pull the eyebrows medially and inferiorly. When the muscle contracts, it creates vertical wrinkles in the glabella area.
This muscle is pierced by branches of the trigeminal nerve, namely the supraorbital and supratrochlear nerves, which supply sensation to the forehead and up to the vertex.
Guyuron and colleagues found that in migraine patients who underwent surgery on this muscle, symptoms improved in 80% of the cases.
This finding sparked the idea that treating peripheral nerves could improve symptoms in migraine patients.
However, like any new treatment, there were differing opinions—some supported it while others were skeptical.
Guyuron coined the term “migraine surgery,” which raised questions about whether patients who improved after surgery truly had migraines and how nerve surgery, targeting the scalp, could relate to migraines.
Historically, migraines were thought to be caused primarily by vascular mechanisms due to their throbbing nature. Additionally, migraines were believed to be linked to the central nervous system, as they often involve auras.
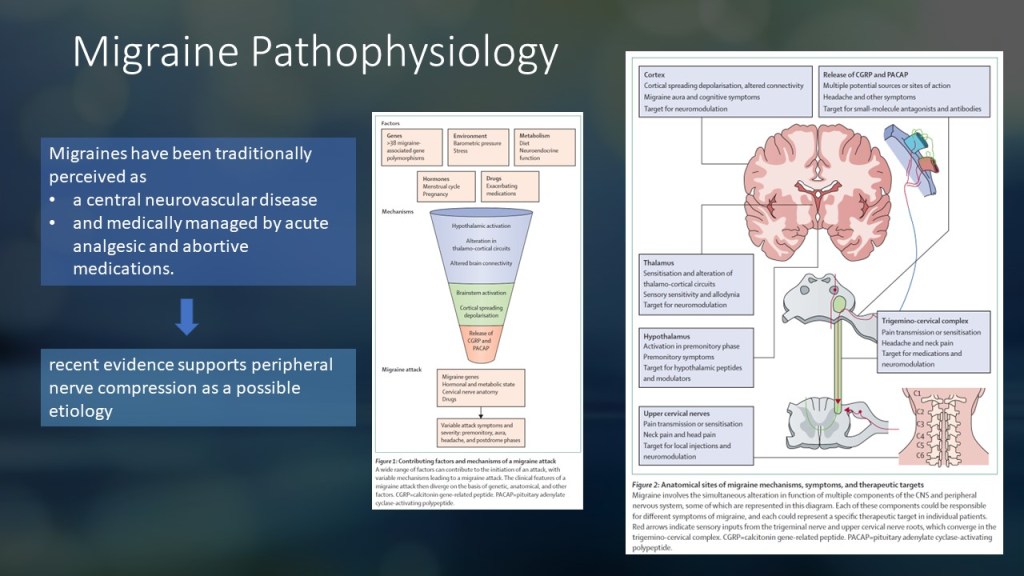
As studies have progressed, it is now understood that the mechanism of migraines is multifactorial, involving genetics, environment, metabolism, and hormones.
Several brain regions, including the cortex, thalamus, and hypothalamus, play a role in the pathophysiology of migraines. Interestingly, the nerves in the upper neck may also contribute to migraine attacks via the trigeminocervical complex.
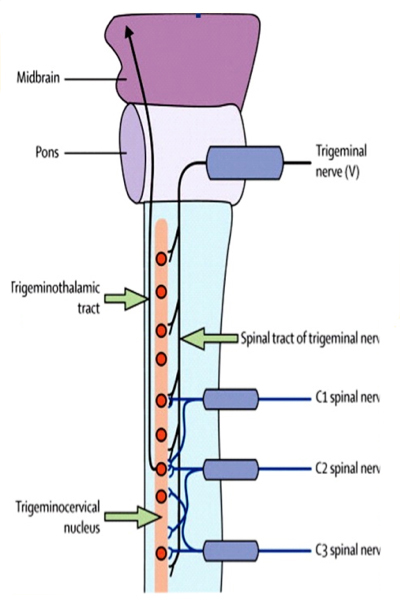
Anatomically, the trigeminal nucleus extends down to the upper spinal cord and is closely associated with the upper cervical spinal nerves.
This theory suggests that targeted treatment of the upper cervical spinal nerves or branches of the trigeminal nerve may have a role in migraine management.
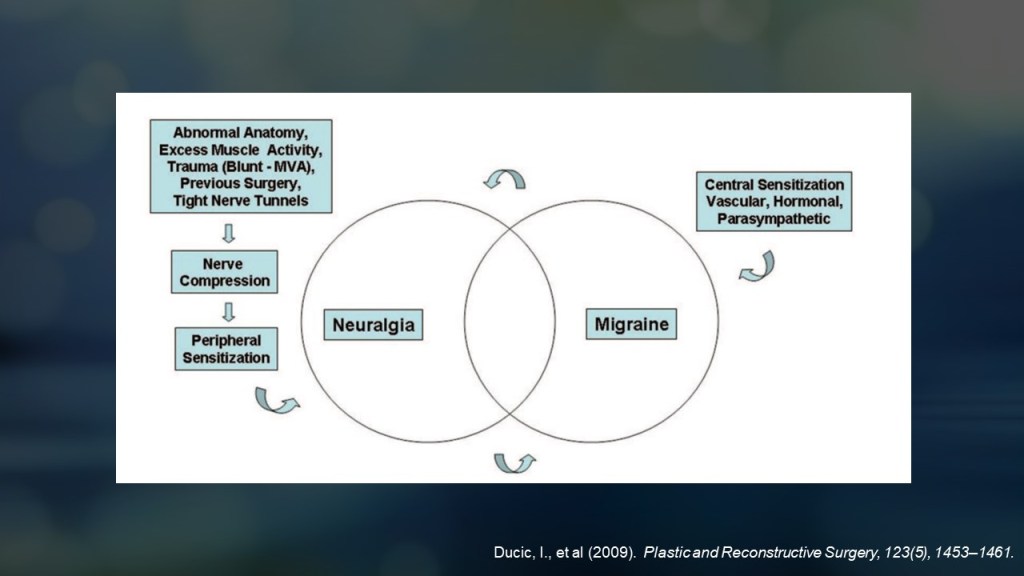
Ducic, a prominent figure in pain surgery, proposed that neuralgia caused by peripheral nerve sensitization overlaps with migraines, traditionally thought to result from central sensitization.
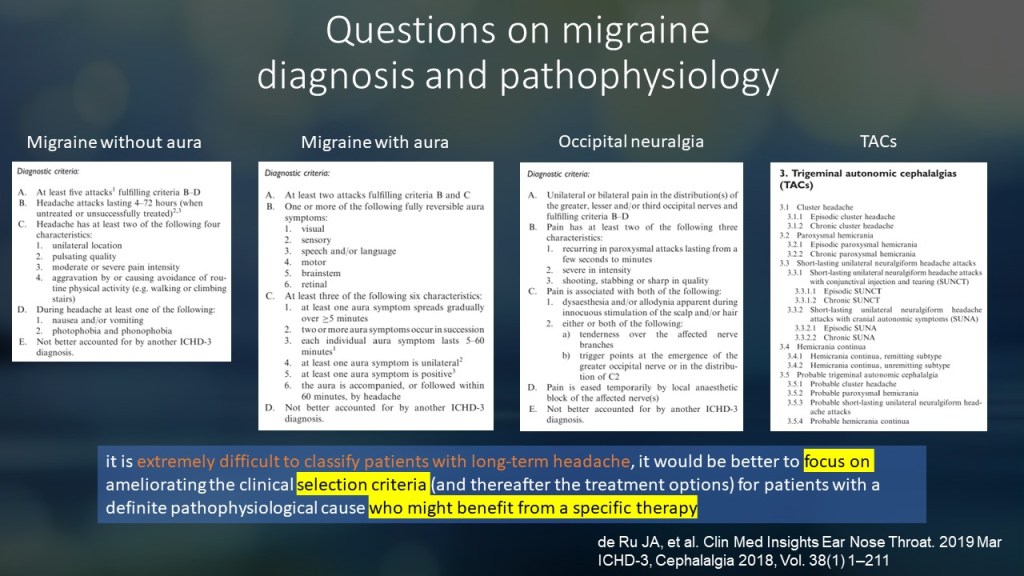
Many experts argue that such conditions should not necessarily be categorized as primary headaches or true migraines but rather as secondary headaches caused by neuralgia.
It has been suggested that many patients with chronic primary headaches are difficult to diagnose precisely using standard criteria. Physicians should focus on selecting the most appropriate treatment for each patient.
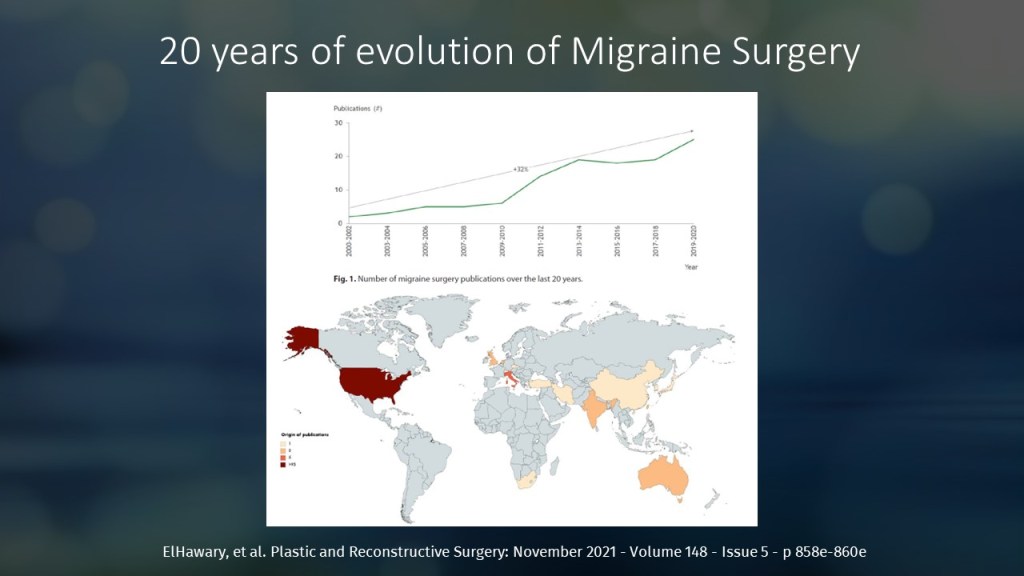
Despite skepticism, research on nerve surgery for chronic headaches has grown significantly over the past 20 years, particularly in the United States.
Key factors contributing to successful migraine surgery can be summarized as PAINS:
- P: Pain point – clearly identifiable tender areas.
- A: Appropriate symptoms – symptoms correlate with the pain location.
- I: Injectable improvement – improvement with nerve block or Botox.
- N: Neurologist-confirmed diagnosis – proper evaluation and diagnosis by a neurologist.
- S: Sketch matching – pain location aligns with the sensory distribution of the affected nerve.
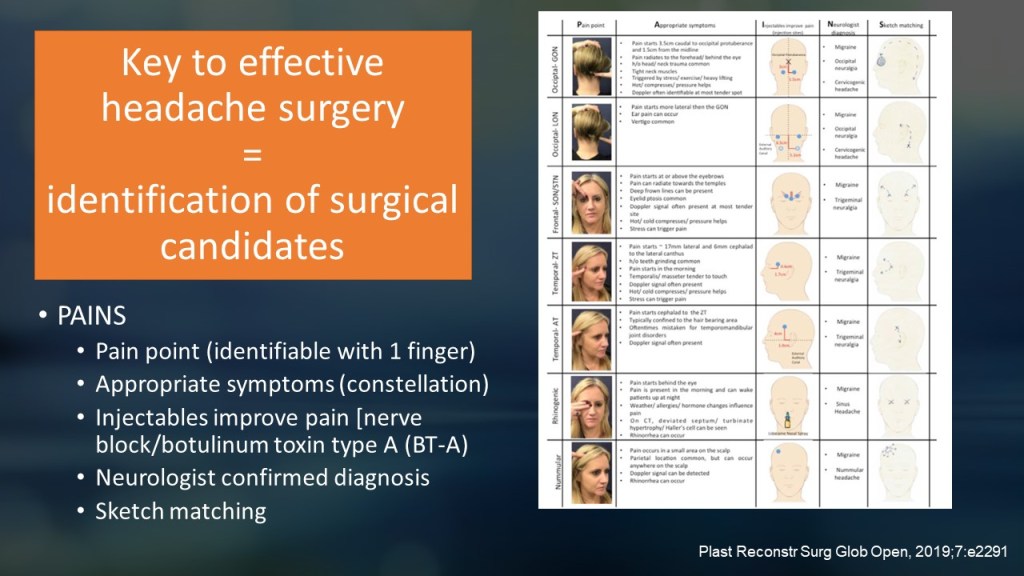
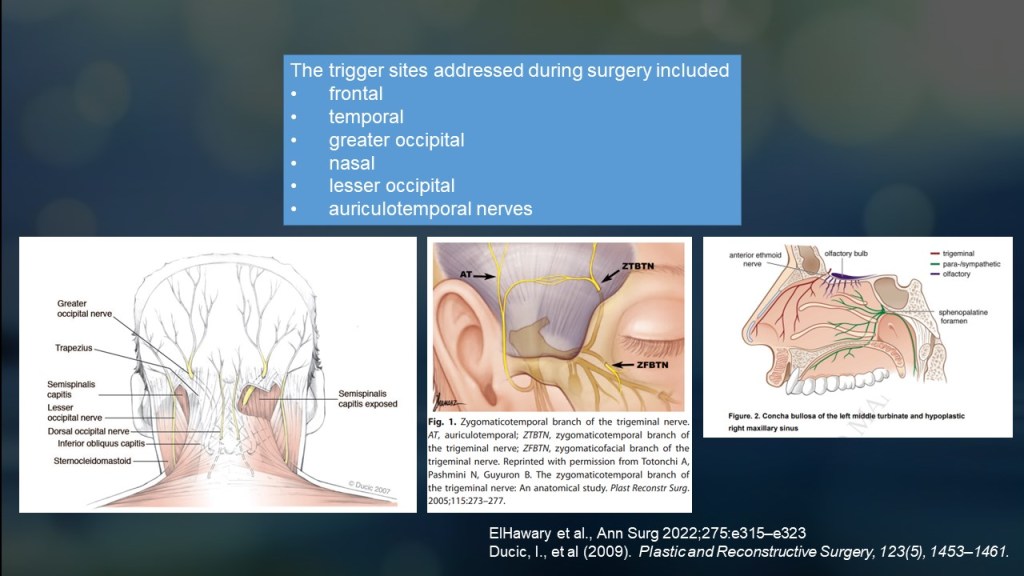
Trigger points are commonly found in the frontal, temporal, occipital, and nasal regions, which correspond to the innervation of specific nerves.
Over the past 20 years, research on migraine surgery has steadily increased.
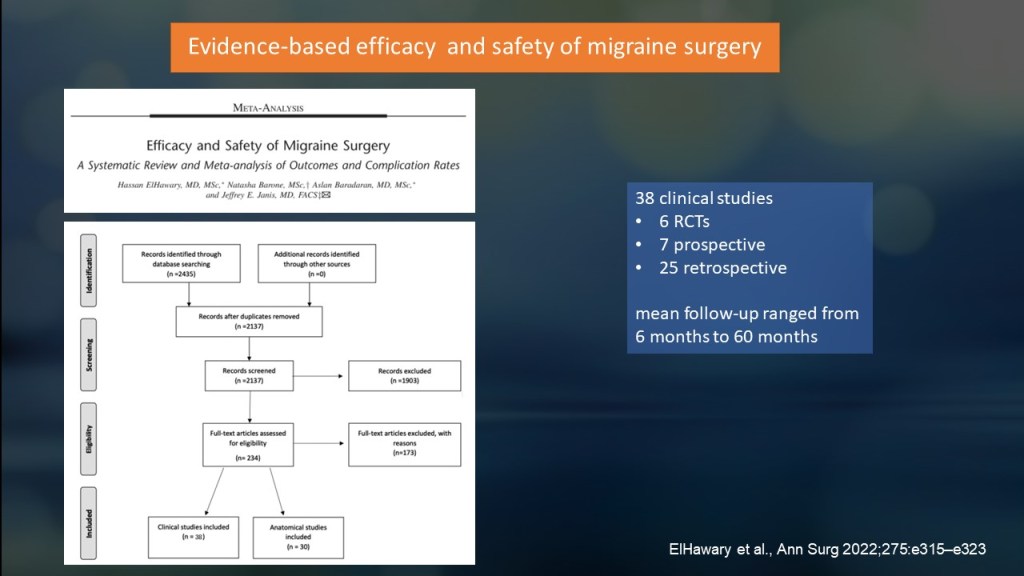
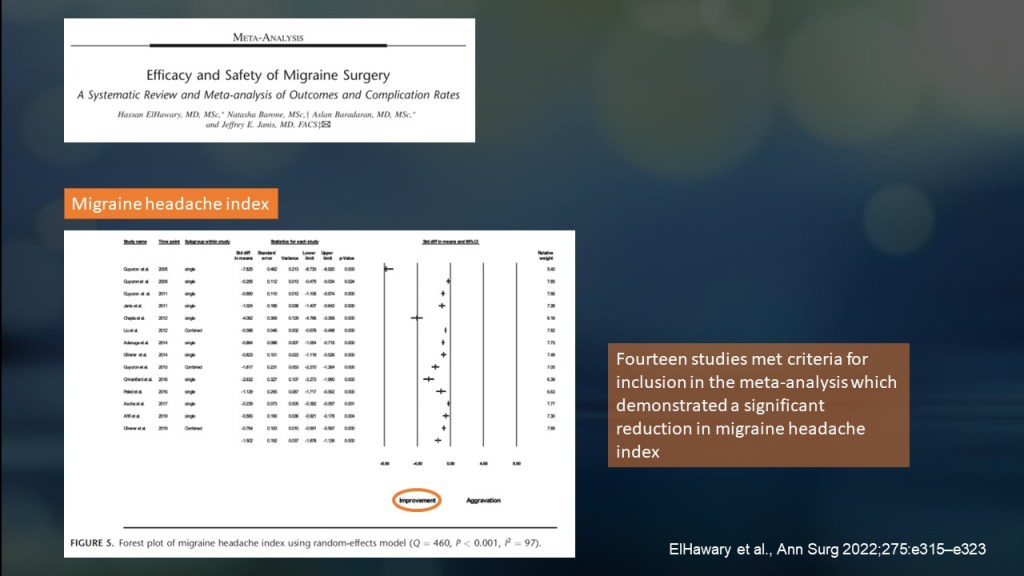
A systematic review and meta-analysis conducted by ElHawary and Janis, pioneers in migraine surgery, provided a comprehensive overview of the field. Published in early 2022, the study included:
- 6 randomized controlled trials (RCTs).
- 25 prospective studies.
- 25 retrospective studies.
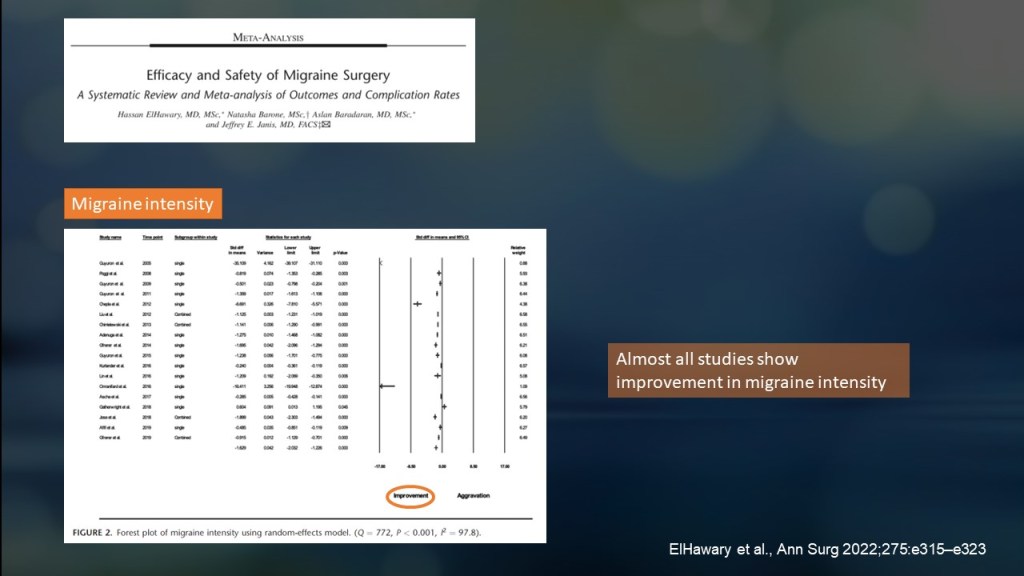
In terms of migraine intensity, nearly all studies included in the forest plot showed that surgery reduced migraine severity. Only one study reported no significant improvement.
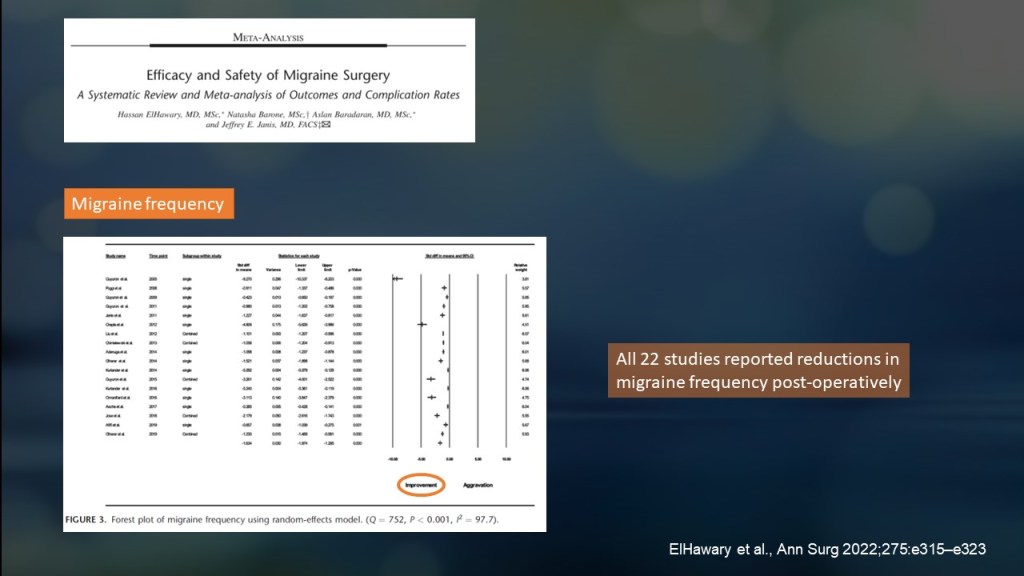
All studies found a reduction in migraine frequency after surgery.
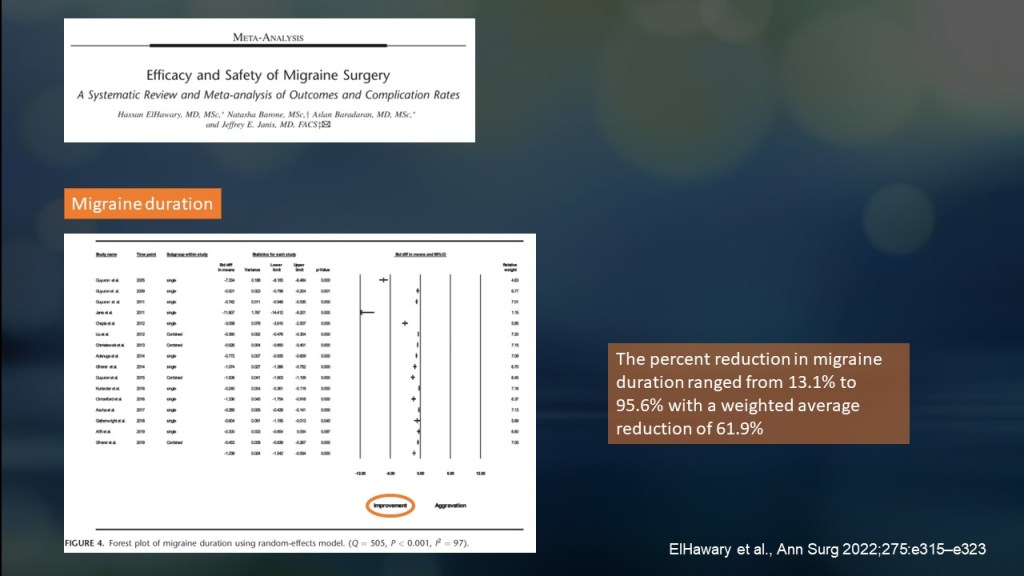
The duration of migraine attacks also decreased, ranging from 13% to 95%, with an average reduction of 62%.
Surgery significantly reduced the migraine headache index (frequency × intensity × duration).
The percentage of patients completely free of migraines after surgery varied across studies, ranging from 8% to 87%.
Most complications from surgery were minor, with the most common being numbness, followed by itching and hair thinning or loss.
The meta-analysis concluded that surgery improves migraine outcomes, reduces the migraine headache index, and is relatively safe.
Summary
Surgery is not the first-line treatment for migraines or chronic headaches. However, it is a viable option for patients who do not respond to medications or other treatments.
The success of surgery depends largely on patient selection—choosing those most likely to benefit.
As surgery is an invasive procedure, the surgeon and patient must discuss treatment options, costs, expectations, and potential complications before proceeding.
So should I do the surgery?
Surgical treatment for migraines should be personalized. Discuss the benefits and risks with your peripheral nerve surgeon to determine if it’s right for you. Contact us for more information.
Disclaimer
This fact sheet is for informational purposes only and is not intended as a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified healthcare provider with any questions you may have regarding a medical condition or treatment options.
The information provided here reflects general practices and may not apply to your individual health circumstances. Outcomes and risks may vary depending on your medical history, condition, and response to treatment.
If you experience any concerning symptoms or side effects following a procedure, contact your healthcare provider immediately or seek emergency medical attention.
This material is not intended to promote or endorse any specific treatment or procedure. Decisions about your healthcare should always be made in consultation with your physician, considering your unique health needs and goals.

Leave a reply to The Mindful Migraine Blog Cancel reply